Sun induced rashes
There are some 20 to 30 of these conditions, one very common but most rare; they are subdivided into groups as described below. Polymorphic light eruption (colloquially called prickly heat) is the common one and is given most attention.
ALLERGIC SKIN REACTIONS TO SUNLIGHT
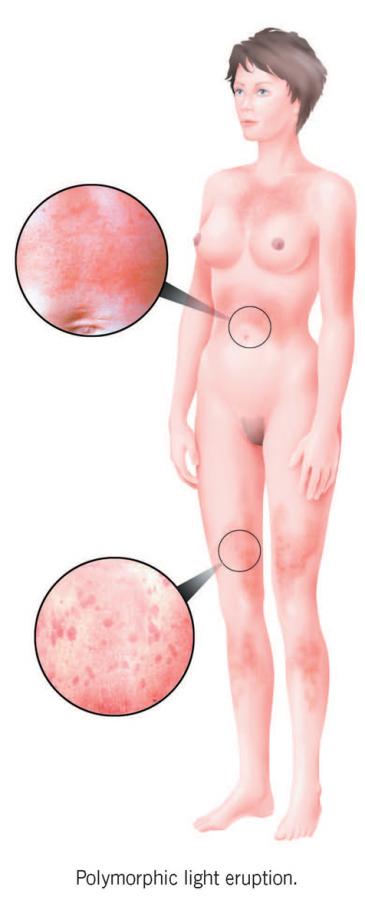
Polymorphic light eruption
About 10 to 15 per cent of people in the UK have this condition, often incorrectly known as prickly heat because it is caused not by warmth but by UV radiation; about five per cent of Australians, 10 per cent of North Americans and 20 per cent of Scandinavians also have it. More women than men are affected, often from adolescence or early adulthood, although children also develop it occasionally and some adults in later life as well. Skin type makes little difference, and black and brown skins are quite frequently affected; there is, not uncommonly, a family history of the condition.
Within minutes to hours of exposing the skin to spring or summer sun, an itchy, red, spotty rash, often like goose-flesh, blisters or hives, develops, often only on some of the exposed areas but usually symmetrically; it frequently doesn’t affect the face or backs of the hands. The outbreak generally lasts for a few days to a week or so before gradually subsiding, provided that the skin is protected from sunlight. Most people just have the problem on very sunny days, or once or twice at the start of the sunny season, or on holidays abroad, but more severely affected individuals may suffer throughout the whole spring and summer.
The exact cause of polymorphic light eruption is not fully understood, but it seems likely that a genetic predisposition leads some individuals to develop a form of immune allergic reaction to normal skin molecules that have been chemically altered by UV radiation and thereby appear foreign to the body. In people who do not have the inherited predisposition, the body apparently fails to develop an allergy to such altered molecules.
Many people with polymorphic light eruption never consult their doctor; either they have learnt to live with it or they avoid strong sunlight. For others, however, it can be an extremely distressing condition. Nevertheless, it is generally readily treatable and, if you are bothered by it, employing one or several of the following measures virtually always works:
• Avoid exposure of your skin to the sun as much as you can.
• Cover up with suitable clothes whenever possible.
• Use a very high SPF sunscreen that also gives very good UVA protection (frequently denoted as a five-star rating), the UVA wavelengths often being particularly important in causing the condition.
• See your GP, if these measures are not enough, for referral to a dermatologist and specialist treatment.
At this stage, the diagnosis must be confirmed because other sunlight-induced conditions, such as lupus, may produce similar abnormalities; none is, however, quite like polymorphic light eruption. After this, particularly if you suffer the rash frequently, you may well be offered preventive UV phototherapy, which, in 60 to 90 per cent of cases, stops the rash for several months to a year or two before further treatment is usually necessary. This therapy comprises a several-week course of twice-weekly, low-dose, artificial UV lamp exposures at the beginning of spring or before a holiday; it is available in many hospitals. Paradoxically, such an approach seems to correct the allergic response by slowly diminishing skin imune reactivity, but is too low in dose to do any harm apart from occasionally inducing the rash temporarily, after which it is often still effective anyway. The treatment course is then repeated if necessary, annually, for the next few years, after which permanent tolerance sometimes sets in.
If the therapy is unavailable, inconvenient, ineffective or unnecessary because of the rarity of attacks, however, a final, usually very useful treatment is to have a corticosteroid injection or course of tablets for several days, both available from a GP or dermatologist, as early as possible in an attack, which will usually settle it rapidly. Such treatment may be used up to about every three months if required; more frequent or lengthy courses have the potential to cause a gradual build-up of side effects and UV phototherapy is needed instead. Brief treatment every now and then rarely causes trouble, indigestion or minimal depression being all that might happen; in this case the medication should be stopped, the adverse effect rapidly disappears and UV phototherapy is again needed.
RARE DNA REPAIR DISORDERS
Xeroderma pigmentosum
Another, extraordinarily rare group of conditions causing sensitivity to the sun is the DNA repair-defective disorders; the most common is xeroderma pigmentosum. This usually causes a strong tendency to sunburn, often with severe blistering after very little sun exposure, and to very early skin photoageing and cancer. The reason for this is that people with the condition cannot effectively repair the skin DNA damage caused by UV radiation exposure as a result of inherited defective DNA-repair genes. If you suspect that one of your children may conceivably have this, see your doctor; treatment is difficult but not impossible.
CHEMICALS, DRUGS AND EXCESSIVE SUNLIGHT SENSITIVITY
Porphyria
A group of rare conditions that are frequently aggravated, but not directly caused, by sunlight is the porphyrias. These are predominantly, but not solely, inherited disorders, the most common being porphyria cutanea tarda. This generally affects people of middle age with symptoms of skin fragility, along with scattered, occasional blistering of sun-exposed skin, usually of the backs of the hands. These changes occur because porphyrins, related to the chemical building blocks of the red haemoglobin pigment in blood, accumulate and absorb light in the skin, thereby being stimulated into damaging the surrounding tissue. It is important to consult your doctor if this seems to be happening to you because the condition is usually treatable; if nothing is done, however, liver damage may slowly develop in some instances. Just occasionally, excessive sunbed use may also cause a similar condition but this never leads to liver damage.
A rarer type of porphyria, which causes a much greater degree of sun sensitivity, is known as erythropoietic protoporphyria (EPP). This generally starts in early childhood and is associated with a very severe, painful, burning skin sensation after UV radiation and visible violet light exposure within minutes of being outside in the summer and lasting hours to a day or so. Again this happens because excessive porphyrin in the skin absorbs the radiation, leading to nearby tissue damage. If a child is too young to tell you that his or her skin hurts, the only sign of this condition might be crying whenever the child is in the sun. Any youngster who often reacts in this way should be seen by the family doctor and if necessary by a dermatologist, in case EPP may be the cause. Treatment is difficult but not always impossible.
Reactions to drugs and creams
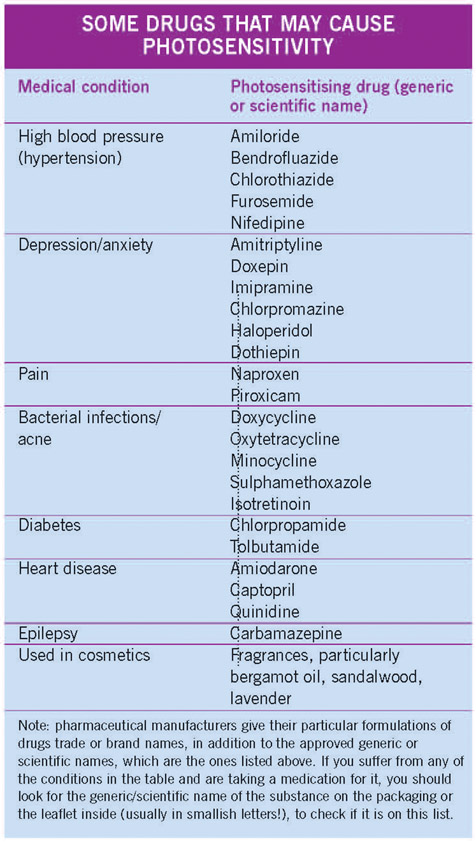
There are a large number of oral medicines and skin preparations that can increase skin sensitivity to UV radiation in a variety of ways. Most usually they cause a sunburn-like inflammation, or sometimes blistering, of skin that has been exposed to the sun, but there may be other problems such as a burning sensation without a rash, skin fragility with scattered blisters, eczema or, very occasionally, nail abnormalities. Generally, the sensitivity develops within days to weeks of starting a new medication, unless perhaps this is in winter and you don’t see much sun for some time; spring is then the time that the trouble usually starts.
Common medications causing such sensitivity are listed in the box on page 64, but there are many others, so if you think that your skin is affected as described after starting a new drug you should consult your doctor. However, many people can take most of these medications without developing sun sensitivity, and those who do often experience only a mild reaction.
The treatment of drug photosensitivity is to change the drug, restrict sunlight exposure, use a sunscreen regularly, or in some cases just take the medication at night if medically appropriate.
SKIN CONDITIONS NOT CAUSED BUT AGGRAVATED BY SUNLIGHT
There are many skin conditions that are not actually caused by sunlight but which may sometimes be aggravated by it, although some are more likely to improve in most individuals after exposure. Some people with even minimal eczema, for example, which is mostly improved by sunlight, find that the sun makes their skin itch more or the eczema worse overall, even in cool conditions. However, it is more common for heat (from the sun, a fire or central heating, for example) to have this effect and, if this happens to you, you may need specialist investigations to determine which sunlight component is actually responsible. Other conditions that may also be aggravated by sun exposure include acne and psoriasis, although again many people who have these find that their skin improves in summer.
No one knows exactly why these conditions are made worse by sunlight in some people, but UV radiation very probably increases the skin immune reactivity, causing the disease in most cases, or rarely may add further sunburn-like inflammation to an already angry skin.
The main approach to therapy is to have careful treatment for the underlying condition, as well as cutting down on exposure to sunlight. Sometimes courses of low-dose preventive phototherapy, as for polymorphic light eruption, may also be helpful, except in people who have lupus (see below), when the condition may instead be made worse.
Lupus
This is a disorder best known for its hallmark, if rather rare, abnormality of a fixed, butterfly-shaped, redness of the nose and cheeks, supposedly giving patients’ faces a wolf-like look (hence the word lupus, which is Latin for wolf). Much more common as far as its light sensitivity is concerned, however, are flat, scaly, sometimes slightly sore red patches, mostly induced by the UVB radiation in sunlight, on other exposed sites. This may be the sum total of the condition, although rarely internal abnormalities such as sore joints or a generalised feeling of being unwell may also occur, again sometimes worsened by sun exposure. The condition is associated with various immunological abnormalities, and one theory of how the rash itself is caused is that skin DNA is changed by the UVB in sunlight enough to cause an allergic reaction, similar to that postulated for polymorphic light eruption.
Treatment of the disorder and rash consists of sun avoidance, the use of strong sunscreens and the application of steroid creams; in addition, a variety of oral medications may also be necessary in severe cases, such as certain so-called anti-malarial drugs, oral steroids, immunosuppressive drugs or even rarely thalidomide. Sometimes the condition may also gradually settle spontaneously.
Vitiligo and albinism
Vitiligo and albinism are both associated with a lack of the protective pigment, melanin, in the skin. They appear as scattered white patches or very rarely pallor all over the body respectively, with a marked tendency to easy sunburning of the affected areas. The best protective advice is to minimise exposure to strong sunlight, cover the affected sites as much as possible with appropriate clothing, and use a high protection factor sunscreen regularly on all exposed abnormal skin. Naturally fair-skinned people with vitiligo will also find this helps prevent the normally pigmented sites from tanning, making the disorder itself less noticeable. Albinos, on the other hand, need to be especially vigilant as they can also develop skin cancer relatively easily if careless in the sun, whereas people with vitiligo usually seem not to, for reasons as yet poorly understood. Albinism is present from birth and is unfortunately untreatable; vitiligo, however, may respond, but sometimes only partly or temporarily, to regular applications of steroid creams or lotions to the affected patches, or else phototherapy, both over a number of months to a year or two.
Melasma
Melasma, or chloasma as it is also known, is a condition most often affecting young and middle-aged women; it is characterised by a patchy brown discoloration, usually of the face, particularly the temples, cheeks and upper lip, and occasionally elsewhere. The exact cause is not known, although a genetic tendency and the female hormone oestrogen seem to predispose to the condition. Other factors appear to be perfume use on affected sites and particularly sun exposure. Some girls first develop the problem around puberty, but the condition is more common soon after a woman starts the oral contraceptive that contains oestrogen or becomes pregnant, which markedly increases oestrogen levels. The discoloration may, although not always, fade once the pill is stopped or pregnancy ceases; minimising sun exposure and sunscreen use also help a little. Skin preparations containing hydroquinone, now only prescribable by doctors, may gradually decrease the colour as well, over months. Skin irritation, allergy and very rarely, after continual use for years, an orangey discoloration called ochronosis can result from using such preparations. However, they frequently work, albeit slowly, and rarely cause trouble in practice.
TREATING SKIN CONDITIONS WITH UV RADIATION (PHOTOTHERAPY)
Although UV radiation is generally harmful to the skin in the long term, there are a number of skin conditions that can be greatly alleviated, albeit usually only temporarily, by its use as a medical treatment. Such conditions may or more commonly may not be caused by sunlight, but those most likely to respond are psoriasis, eczema, cutaneous T-cell lymphoma (a rare skin cancer), vitiligo and polymorphic light eruption, although a whole host of others may sometimes do so as well. When used in this specific way, the benefits of UV radiation in a particular individual are considered in discussion with him or her to outweigh the potential risks, even though the treatment does inevitably involve some overall damage to the skin. The situation is discussed in some detail with the patient beforehand and the treatment, which can generally be used only for a limited period, probably about two years, in total because of the potential build-up of side effects, is given only with the patient’s written consent.
There are two main types of such UV radiation treatment:
• UVB phototherapy, which is given alone, as either so-called broad- or narrow-band UVB, which refers in each case to the breadth of the wavelength spectrum emitted by the lamp.
• Psoralen and UVA photochemotherapy (PUVA), which is a combination of a photosensitising medication called psoralen, given beforehand, followed soon after by broad-band UVA exposure.
UVA radiation without the psoralen, which is broadly what many sunbeds deliver, is usually many times less effective at treating skin disease than either UVB or PUVA, but still damaging overall to the skin, and you should not therefore generally use self-therapy with these devices as a substitute for the carefully medically supervised approach.
Before your doctor decides to offer you phototherapy for a skin condition, he or she will carefully assess you to make sure that to all intents and purposes it will be relatively safe. You will therefore be asked whether you are on any drugs or medications that might increase your UV sensitivity, whether you have had much previous sun exposure and whether you have ever had conditions such as polymorphic light eruption or skin cancer. Your doctor will then explain the advantages and possible risks of the treatment, which include a small chance of burning, and a very gradually increasing risk of photoageing and skin cancer if the therapy should need to continue over a number of years. These risks are, however, well documented nowadays and the radiation doses recorded accurately to ensure maximum safety. The twin aims of medical supervision are thus to keep each treatment dose below that causing sunburn and to ensure that the cumulative (or lifetime) dose is also as low as possible, thereby minimising the long-term risks.

It is not known for certain how phototherapy improves those conditions that are responsive to it. However, psoriasis and eczema seem to be disorders in which the skin immune system is overactive, thereby causing the characteristic rash. Phototherapy appears to diminish this response, probably by damaging skin immune cell DNA and altering subsequent immunological pathways. In addition, it may also slow down the excessive epidermal basal cell growth of psoriasis and thus reduce the skin overgrowth of the disease; again, it probably does this by its effect on cellular DNA, this time in the basal cells. In cutaneous T-cell lymphoma, a rare but usually mild form of widespread skin cancer not caused by sunlight, phototherapy is again very helpful, also probably by damaging tumour cell DNA and growth.
In vitiligo, another disorder that is sometimes responsive to phototherapy, UV radiation exposure again probably damps down abnormal immune activity affecting the skin tanning cells – very possibly a major causative factor in vitiligo – while also stimulating melanin production in those melanocytes still functioning. However, photo-therapy is not always effective in this condition, some individuals responding too slowly or poorly, whereas others may tend to relapse and need continuing treatment; the long-term risks of the therapy may then outweigh the benefits. In practice, therefore, it seems that phototherapy is most suited to vitiligo patients with dark skins and relatively few and small affected patches, particularly of the face or trunk.
Finally, the photosensitivity disorder, polymorphic light eruption, probably an immunologically mediated condition as well, also responds, in this case usually very satisfactorily, to short preventive courses of low-dose phototherapy, as already described. This is also probably mediated through changes in the skin’s immune response.
